What is trigger finger?
Finger locking, also known as finger springs or spring fingers, is a medical condition where a finger or thumb becomes difficult to bend or unfold due to a sudden, uncontrollable contraction of the flexor tendons. When the finger bends, it may appear to remain stuck in a bent position, then suddenly unlock with a sudden movement, hence the term “springing”.
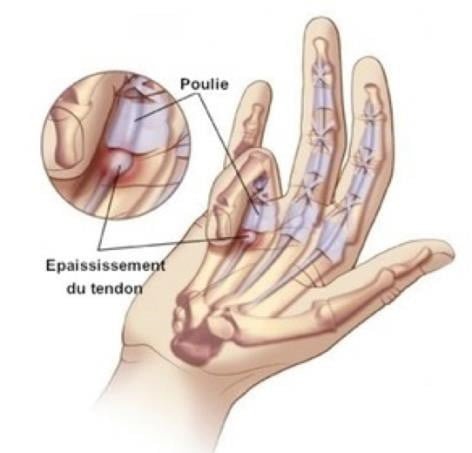
This condition is usually caused by a thickening or nodule in the flexor tendon, which causes abnormal friction against surrounding structures during finger movement. This can lead to temporary blockage of finger movement, followed by sudden release.
The tendon’s ability to glide smoothly becomes impaired, accompanied by initial discomfort followed by sporadic episodes of blockage. Initially, these blockages occur on waking in the morning, due to the tendon catching on the palm. The recurrence of these blockages leads to inflammation of the tendon, increasing friction and aggravating the syndrome.
What are the signs and how is the diagnosis made?
Club finger syndrome is a common cause of finger pain.
Characteristic symptoms include temporary, painful episodes of locking when moving a finger from flexion to extension. As the condition progresses, blockages are accompanied by stiffness of the finger and reduced range of motion. In advanced cases, the protruding finger may lead to complete locking in flexion or extension (often seen in the thumb).
This condition can affect one or more fingers simultaneously or successively, and can also affect both hands.
It’s important to look at certain contributing causes, such as rheumatic diseases or diabetes.
Protruding fingers can also occur after carpal tunnel syndrome surgery, without necessarily being a complication.
A particular variant of the jagged finger manifests itself in childhood as a congenital flexion block, mainly in the thumb.
What additional tests are required?
In general, no further examination is necessary, as the diagnosis of a club finger is based primarily on clinical examination.
However, in cases where symptoms are still at an early stage and manifest themselves mainly as pain with no obvious protrusion, an ultrasound scan may be considered. This would detect any inflammation of the tendon sheath and the presence of effusion.
In summary, the diagnosis of club finger is usually established by clinical examination, but additional tests such as ultrasound may be used in certain situations to confirm or assess the severity of the condition.
What is the treatment?
Treatment is prescribed when protrusion phenomena cause functional discomfort. Initially, treatment may be medical in nature.
This involves administering infiltrations of powerful anti-inflammatories (corticoids) into the tendon sheath, precisely in the area where the blockage occurs, following strict asepsis rules.
This approach is effective in early cases, although symptoms may reappear over time. Generally, one or two infiltration treatments can be envisaged.
In situations where symptoms are more pronounced, surgery may be considered as a first-line option when “pseudo-blockages” occur (requiring the help of the other hand to unblock the finger) or in cases of joint stiffness. It may also be considered at a later stage if medical infiltration fails.
The operation is generally performed on an outpatient basis under local anaesthetic. It involves a small skin incision in the palm to partially open the tendon sheath and pulley at the site of the blockage. If significant inflammation is observed during the procedure, further excision of the tendon synovium may be required.
By keeping the pulley open, recurrence of symptoms is generally avoided. Following nursing care for around two weeks, normal use of the finger is encouraged.
In some cases, re-education sessions can speed up recovery of finger mobility, particularly when stiffness was a problem prior to surgery.
The length of time off work depends on the patient’s occupation.
What complications could arise?
This is a relatively simple surgical procedure, with specific risks that are not very frequent. The scar may remain tender or swollen for the first few weeks.
The risk of hematoma is rare, and spontaneous resorption is normally expected.
The most common complication is finger stiffness, either pre-existing before surgery, or developed afterwards due to limited use of the finger. In such cases, rehabilitation sessions and the use of a dynamic device may be required. As with any surgical procedure, there is a risk of haematoma, which usually resolves itself, but in rare cases an evacuation puncture or surgical drainage may be necessary.
Infection is exceptional. If it does occur, it may require further surgery and prolonged administration of antibiotics. Edema is frequently observed, causing painful discomfort and making finger mobility difficult.
Algodystrophy is rare: it’s a painful, inflammatory phenomenon that’s still poorly understood. It is treated medically and can persist for several months, even years. Its management involves appropriate rehabilitation, additional tests and, in some cases, specific pain management. The manifestation and evolution of algodystrophy are unpredictable, and may leave potential sequelae.