A wrist fracture is a break or crack in one of the bones that make up the wrist region. The wrist is a complex structure made up of several small bones called the carpal bones, as well as the forearm bones, ulna and radius. A wrist fracture may involve one or more of these bones.

Location from radius (at top) and from the ulna (at bottom) by report à the hand. A fracture from wrist concerns usually the part from radius which go to visit from at from the hand.
Qu‘is a bonesteosynthèse d‘une fracture du radius distal ?
The aim of internal screw-plate fixation is to realign and stabilize the distal radius fracture and restore the normal anatomical configuration of the wrist, if feasible. These plates are positioned in contact with the bone through a surgical incision that requires a skin opening. They can be implanted on either the dorsal or ventral side of the wrist, although the ventral side is more frequently chosen.
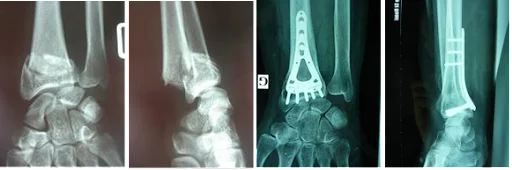
Example from fracture from wrist moved and a plate from wrist such it go to position on the face previous from radius distal
Before the operation
Imaging assessment is based on X-rays, and in some cases a CT scan may be added in the case of a complex fracture to obtain more detailed information.
The intervention
Occasionally, management of a wrist fracture may be delayed by a few days, due to factors such as the need for further tests, scheduling of the operation, or severe swelling. In such cases, a temporary immobilization splint is usually applied pending surgery.
Surgery is usually performed under local anaesthetic, which is determined during consultation with the anaesthetist. The surgeon makes an incision on either the palmar or dorsal side of the wrist. The aim of the operation is to realign the fracture (restore normal anatomy), before fixing a plate to stabilize the fracture and promote healing. The use of an image intensifier (real-time X-rays) is usually performed during the procedure to guide the precise positioning of the plate.
In certain situations, other devices such as pins or an external fixator may be used in addition, depending on the nature of the fracture and local characteristics.
Intraoperative arthroscopy may also be performed during surgery. This involves inserting an optical tube fitted with a camera into the wrist to assess the quality of fracture reduction, particularly in the case of articular fractures. In addition, arthroscopy can be used to search for any ligament lesions not visible on X-rays.
Post-operative care
Hospitalisation for a wrist fracture can be either outpatient (you go home the same day as the operation) or for a few days as a full hospitalisation. Finger mobilization is generally permitted immediately after surgery.
The monitoring of dressings, pain management and follow-up appointments will be adapted to each individual case and will be indicated by your surgeon.
Temporary immobilization in the form of a splint or cast may be necessary, but is not systematic. The duration of immobilization will depend on the nature of the fracture, the specific conditions of your case and the stability of the fixation.
In many cases, rehabilitation will be recommended, either immediately after surgery or at a later stage. The duration of rehabilitation can vary considerably, from several weeks to several months, depending on the severity of the fracture, the procedure performed and your individual progress.
Complications
The most common complications that can occur after wrist fracture surgery include:
- Hematoma: As with any surgical procedure, there is a risk of hematoma, which generally resolves spontaneously. In rare cases, it may require puncture for evacuation or surgical drainage.
- Deep infection: Deep infection is exceptional, but if it does occur, it may require further surgery and prolonged antibiotic treatment.
- Smoking: Smoking is strongly discouraged during the healing period, as it increases the risk of infection and delays healing.
- Edema: Swelling of the operated area is common and may cause discomfort and difficulty in moving the fingers. Elevating the wrist and applying ice can help reduce swelling, but it may take several months to resolve.
Less frequently, the following complications may occur:
- Nerve or tendon damage: Nerve or tendon damage is rare, but may require additional surgery to correct the problem.
- Algodystrophy: This is a poorly understood painful phenomenon that may require medical treatment and specific rehabilitation. It can last several months or even years, and its after-effects can vary.
- Scars: Scars may remain swollen and tender for several weeks.
- Stiffness and limited mobility: Temporary stiffness of the wrist may occur, requiring further rehabilitation. A permanent reduction in wrist mobility may also occur, depending on the severity of the fracture and the intervention.
- Sequellar deformity: Sequellar deformity of the wrist, such as callus, is rare but can occur.
- Ligament damage: In the case of articular fractures of the distal radius, associated ligament damage may require subsequent intervention.
- Delayed consolidation or pseudarthrosis: This is very rare, but in some cases, bone consolidation may be delayed or fail to occur properly, necessitating further treatment or intervention.
- Hardware-related complications: Problems with the osteosynthesis hardware, such as tendon conflicts, can occur. In some cases, removal of the hardware may be necessary.
It’s important to note that each case is unique, and the risk of complications can vary depending on many factors, including the nature of the fracture, the surgical technique used and the individual characteristics of the patient.
Results to look forward to
Internal plate fixation of a wrist fracture is a well-defined surgical procedure. Progression and final outcome are subject to great variability. Sequelae may persist due to the type of fracture or other unpredictable factors.